
{kind=link}
Way, way back in 2007 or so, a friend of mine, Dr. Mark Hoofnagle, coined the term “crank magnetism” as a pithy phrase to describe a very simple concept, specifically that those who tend to believe one piece of pseudoscience, quackery, and/or conspiracy theory (e.g., antivax pseudoscience and conspiracy theories) will often also be attracted to—and come to believe in—other forms of pseudoscience (various forms of quackery, such as “autism biomed,” alternative medicine, evolution denial, HIV/AIDS denial, and more). These beliefs are often—but do not have to be and often are not—related to each other; they can even be mutually contradictory. The term also describes the tendency of even “one-issue” cranks and conspiracy theorists to accumulate more conspiratorial beliefs over time. It’s almost as though, once one’s brain is “opened” enough so that one’s brains fall out, it’s a two-way street, with that opening allowing all manner of nonsense to enter as well. We’ve definitely seen the same phenomenon play out in a huge way since COVID-19 hit and the disease minimizing, anti-public health, “miracle cure” (e.g., hydroxychloroquine, ivermectin) pushing conspiracy theorists joined forces with antivaxxers before there even was a vaccine against COVID-19, which brings me to Tess Lawrie, who reminded me of this last week with a post on her Substack titled “Can cancer really be cured with ivermectin and other safe, old treatments?” This post reminded me instantly of Mark’s old phrase, while providing an “in” to discuss not only how general conspiracism has spread throughout the COVID-19 minimization/antivax movement while at the same time looking at the claim made in this post.
And if that weren’t enough, the tagline to Lawrie’s post got me:
Big pharma will say no – but this cancer survivor and TOP scientist knows otherwise
Yep, it’s the cures “They” don’t want you to know about—shades of Kevin Trudeau! Also, the all caps on the word “TOP” just made me chuckle. Moreover, as you will soon see, linking Jane McLelland’s story to ivermectin turns out to be a bit of a “bait-and-switch.” I’ll explain later in the post and as indicated in this “teaser“:
Jane’s own diagnosis and treatment began back in the 1990s and she describes the amazing support she received from her doctors at the time. It seems that when she would suggest a particular drug or protocol, they would be open to the idea, and agreed to let her just try.
So McLelland’s cancer was diagnosed nearly three decades ago, long before the pandemic hit and ivermectin as a miracle cure for COVID-19 became a thing. So where does ivermectin even come in? Patience. Before I get to that, though, I think it’s important to recap Dr. Lawrie’s past activities with respect to ivermectin.
Before cancer, Tess Lawrie hawked ivermectin as a cure for COVID-19
Regular readers might remember that we at SBM have written about Tess Lawrie before, mostly in 2021, as she became a leading voice in promoting ivermectin against all evidence as a miracle treatment for COVID-19, leading me to quip that ivermectin is the new hydroxychloroquine in multiple posts, based on how, as high quality randomized controlled trial (RCT) evidence failed to find a significant treatment effect for hydroxychloroquine, COVID-19 “miracle cure” advocates switched to ivermectin and spun all manner of conspiracy theories about why “They” kept denying that it was a cheap, safe, and highly effective treatment for COVID-19. What was predictable about Lawrie is how she denied being an antivaxxer but by last June was appearing at the antivax Better Way Conference with Dr. Robert “inventor of mRNA vaccines” Malone, Bret Weinstein, Geert Vanden Bossche, Jessica Rose, and even Robert F. Kennedy Jr. supposedly in attendance, leading Tim Hume to describe the meeting as the “Davos of conspiracy theorists.”
I don’t want to rehash a lot of what I’ve written about in detail before, but I do think it important to point out that early in the pandemic hydroxychloroquine, a repurposed malaria drug that also has mild immunosuppressive activity that makes it useful to treat rheumatoid arthritis, was recommended, based on no high quality (or, truth be told, even moderate quality evidence) as a first line drug to treat COVID-19. As I’ve described a number of times, this was based on a report out of Wuhan in early 2020 from Chinese physicians that none of a group of 80 patients with rheumatoid arthritis taking hydroxychloroquine caught COVID-19. As a result of that and old in vitro evidence of antiviral activity, they became interested in using these antimalarial drugs to treat COVID-19. Based on anecdotal reports and small preliminary clinical trials, in March 2020 the Chinese government published an expert consensus recommending chloroquine or hydroxychloroquine for patients with COVID-19. Soon after, a number of nations followed suit. From there, a French “brave maverick scientist” named Didier Raoult—remember him?—latched onto the drug as the “answer” to the COVID-19 pandemic, publishing risibly bad studies claiming to show its efficacy. Tech bros such as Elon Musk discovered the claims about hydroxychloroquine and Raoult’s bad science, leading to Donald Trump Tweeting favorably about his study and, ultimately, to the FDA issuing an emergency use authorization for the drug to treat COVID-19 that it was forced to revoke by the end of April 2020, and by summer 2020 it was very clear that hydroxychloroquine was not only not a “miracle treatment” but almost certainly ineffective, all the familiar-sounding—to SBM readers, anyway—“miracle cure” anecdotes touted by Fox News personalities notwithstanding.
An old pal in Los Angeles (no Trump fan) just texted me that seven friends of hers (here and in Sweden) ALL took hydroxychloroquine, all recovered quickly, zero side effects. Called it a “godsend.”
— Laura Ingraham (@IngrahamAngle) April 10, 2020
Enter ivermectin, a drug that is highly effective in treating parasitic diseases of human and animals due to roundworms (helminths). Based on in vitro studies showing activity against SARS-CoV-2, the coronavirus that causes COVID-19, advocates like Tess Lawrie latched onto ivermectin as the new hydroxychloroquine; i.e., a cheap, safe, and effective treatment for the disease. The problem with this claim was obvious right from the beginning to anyone who applies science-based approaches to medical problems. As I discussed, the concentration needed to inhibit SARS-CoV-2 in cell culture is at least 50 times higher than what can be safely reached in the bloodstream. Just from a pharmacokinetics and pharmacodynamics standpoint, it was always a highly implausible hypothesis that ivermectin would be an effective drug for prevention, postexposure prophylaxis, or treatment of COVID-19, and eventually RCTs showed that it isn’t any of these things. It doesn’t work, leading me to call it the acupuncture of COVID-19 treatments and use it as an example of why science-based medicine isn’t just for “integrative medicine,” but for all medicine.
In any event, Lawrie is one of the founders of a UK group known as the BIRD Group, which exists mainly to promote ivermectin as a miracle cure for COVID-19. Just take a look at the landing page of its website in June 2021:
Nope. No bias here. Perish the thought!
And here is what it looked like yesterday as I was writing this:
Same as it ever was!
When it comes to the BIRD Group and ivermectin, apparently 2023 is the new 2021.
Now, on to the crank magnetism.
Ivermectin: A miracle cure for cancer?
With that background out of the way, let’s take a look at Lawrie’s post from Thursday and the claims made there. First, Lawrie leads with the antivax myth that COVID-19 vaccines cause cancer (or “turbo cancer,” as they sometimes call it) to set up her narrative:
As we covered back in December, researchers and oncologists like Professor Angus Dalgleish are seeing a disturbing proliferation of cancers, in particular following Covid injection. Even before the pandemic, the incidence of cancers was increasing and a recent study has found that the occurrence of brain cancer is related to both GDP and mobile phone usage.
Actually, no. There is no good evidence that cell phone radiation causes cancer, particularly given how there is no good physical or molecular mechanism that would explain how it might do so. I might have to look into that study more, but I can tell from the abstract alone that there are a lot of caveats there. In the meantime, it’s not surprising that Lawrie is moving into more crankery:
Today, I want to focus on what on earth we can do about it. To help me, I’m consulting not an oncologist, or a pathologist, but an exceptional woman who became an expert by necessity. She’s called Jane McLelland and her knowledge in this area is worthy of a PhD.
Jane is one of several people I have met in the last three years who are top scientists, just without the long line of initials after their names. Her own Stage IV cancer diagnosis forced her down a path of inquiry and investigation – and this research quite literally saved her life. That was about two decades ago, and she’s been helping others ever since.
As I say whenever I discuss alternative medicine cancer cure testimonials—and, make no mistake, that’s exactly what Ms. McClelland’s story is, an alternative medicine cancer cure testimonial—I always preface them by saying that I’m happy the person is doing well and so far surviving her cancer. Always. As a cancer surgeon myself, I don’t wish cancer on anyone, and I particularly don’t want anyone to die from cancer. Unfortunately, however, Ms. McClelland, Dr. Lawrie’s claim that she is a “TOP scientist” notwithstanding, is a fake expert, who claims that her self-discovered knowledge trumps that of experts who have formal training and have devoted their lives to studying cancer and/or treating cancer patients. For one thing, she has no training in oncology or scientific research, being a Chartered Physiotherapist who worked in the UK’s NHS and private practice for twelve years, specialising in Neurology and then Orthopaedic.
Does this sound familiar at all? Similarly, does this part about how “They” don’t want patients to have access to ivermectin, which in the video clip included McLelland claims to be also highly effective against triple negative breast cancer (TNBC)—and that’s my area of expertise!—to cure their COVID-19?
Of course it does:
When the pandemic was at its height, we were inundated with pleas from people who were desperate to get ivermectin to their loved ones in hospital, but who were blocked at every turn. Doctors and hospitals would not even entertain the idea of trying this safe medicine, even when a patient’s prognosis was poor and there was little to lose. In our conversation, I mention one instance where we quite literally helped smuggle ivermectin in a chocolate bar to a woman in intensive care:
It makes me wonder: if this pandemic had arrived in the mid-nineties, it might well have been over within a few weeks. I imagine word would have spread that ivermectin, together with other nutraceuticals such as vitamins D, C, quercetin and zinc, were doing the trick and that would have been that. How things have changed!
Of course, it couldn’t possibly have been all the supportive care in the hospital that saved her—I wonder if she got monoclonal antibodies—but of course it had to be that single dose of ivermectin smuggled to her in a chocolate bar. Let’s just say that when someone’s lungs start getting better it can sometimes happen faster than expected. This reminds me very much of testimonials attributing “miracle cures” to hydroxychloroquine that were circulating early in the pandemic, such as one from April 2020 from a local Michigan State Representative named Karen Whitsett, a New Jersy man named Billy Saracino, and an Alabama man named Carl Shuck (who was still on a ventilator for two weeks), all of whom I discussed at the time and explained why they weren’t good evidence that the drug worked. As I said at the time, were we to believe the media accounts, if you receive hydroxychloroquine (±azithromycin) and recovered, no matter how much time it took, obviously it was the drugs that had cured you. Such was the narrative the media was feeding the public, and such is this narrative. Indeed, I explicitly likened these narratives to the “miracle” cure narratives for Stanislaw Burzynski’s antineoplastons and other alternative medicine “miracle cure” cancer testimonials.
Nor could it have been all the other treatments that Jane McLelland used in addition to ivermectin, which, as you will see, struck me as a small part of the numerous dubious and quack treatments that she used. The similarities between ivermectin miracle cure testimonials and cancer miracle cure testimonials couldn’t be more clear, though. If a patient used a bunch of other treatments plus the miracle cure, it must have been the miracle cure that made the difference. Again, we’ve seen this phenomenon before—and I’ve discussed it more times than I can remember since 2008—with miracle “cures” for cancer, autism, and, yes, COVID-19.
Jane McLelland’s story
So let’s look at Jane McClelland’s “miracle cure” testimonial for ivermectin, as described both in her post from Thursday and from Sunday, the latter of which is titled “How to starve cancer” (a title that, unsurprisingly, caused my cancer quackery detection antennae to start twitching even more furiously than they had been twitching after the first article) and includes a video interview. I sighed when I realized that the interview is over 40 minutes long because I realized that I was going to have to watch the whole thing in order to discuss her testimonial in detail. However, going in I couldn’t help but note this part:
Here are just a few highlights:
- A ketogenic diet can help starve cancers – but diet alone rarely works. It’s also important to be careful about the type of fat you consume.
- The skin of sweet potatoes has anti-cancer properties – so no more binning the peel!
- Cancer tries to find different routes to feed itself – so it’s essential to block all pathways, not just one.
- Different cancers will use different, dominant pathways, so the treatment strategy must be tailored accordingly
- Safe, effective, repurposed drugs such as ivermectin are an essential element of blocking the right pathways – but they’re usually overlooked (surprise, surprise)
- Cancer stem cells are unaffected by chemo and radiotherapy, so they’re left behind to seed new tumours. It’s essential, then, to target these – Jane explains how
- Ferroptosis is a strategy that effectively weaponises cancer’s need for iron, stopping it in its tracks
This is a rich conversation with so much valuable information and I learnt so much speaking with Jane. Please feel free to share with anyone you think may benefit.
Once again, which is it? I’ve discussed how claims for ketogenic diets—which have even been claimed to “beat chemo for almost all cancers” are overblown at best and completely wrong at worst and have even noted how ketogenic diets have been associated with decreased quality of life in cancer patients; so I won’t dwell on that much. I will give her credit; like so many non-experts, she has learned the language. I will admit that, prior to this, I had been unaware that cancer quacks had latched onto ferroptosis, as well, and her mention of it actually piqued my interest because in an effort to restart my lab, which did not do well during the pandemic, I recently started collaborating with an expert on ferroptosis. Of course, like so many cancer quacks, Ms. McLelland knows the lingo but doesn’t really understand it. In this way, she reminds me of Dr. Stanislaw Burzynski, who in addition to his antineoplastons developed something he called “personalized gene-targeted” therapy, which when I examined it turned out to be basically a “throw everything but the kitchen sink at it” approach to cancer, in which he used a bunch of very expensive targeted therapies without much thought about how they might interact, all while claiming he was better at personalized cancer therapy as M.D. Anderson Cancer Center—and had even invented it.
I’m also going to point out that in the clip included in Dr. Lawrie’s very first post, McLelland made a statement that is, to put it kindly, completely wrong. Remember where I mentioned that she claimed that ivermectin is a “fantastic drug” for cancer, specifically TNBC? Right after that, she claims:
I suggest that people look at that [ivermectin] particularly for things like triple negative breast cancer, where the breast cancer is known to be a “cold” tumor; so it doesn’t respond to immunotherapies. But if you take ivermectin it becomes a “hot” cancer that does respond to immunotherapies, and this is a big thing. You know, if we could get more people to take more immunotherapies that could work, that is a big potential step forward. So ivermectin for triple-negative breast cancer works very well and is in fact synergistic with our ferroptosis protocol as well. Ivermectin I love for various factors; it really targets the EGFR mutations and HER2, which is very commonly associated with breast cancer and other cancers that use the HER2 as well.
TNBC doesn’t respond to immunotherapy? TNBC are “cold” tumors that the immune system doesn’t recognize? Quite the opposite, at least for a large subset of TNBCs! I’d like to refer Ms. McLellan to the KEYNOTE-522 clinical trial published in 2020 and NCCN guidelines, which showed that adding pembrolizumab (KEYTRUDA) to standard-of-care neoadjuvant chemotherapy (chemotherapy before surgery) resulted in a significant increase in the pathological complete response rate (the percentage of patients whose surgical specimens contain no residual tumor detectable by pathologists looking at them through the microscope) and benefited even patients with metastatic disease if their tumors expressed the protein PDL-1 Of note, pembrolizumab is an immune checkpoint inhibitor, and immune checkpoint inhibitors are considered immunotherapy. In fact, the use of this immune checkpoint inhibitor is now standard-of-care for operable TNBC. (For those of you not familiar with TNBC, this subtype of cancer lacks the receptors estrogen and progesterone hormones, as well as the HER2 oncoprotein, and tends to be more aggressive than hormone receptor-positive cancers.) Let me say that again. Chemoimmunotherapy is the new standard of care for TNBC since 2020.
Conveniently enough, I encountered this illustration on Twitter of KEYNOTE-522:
Here's the EFS endpoint from KEYNOTE-522. 7.4% absolute improvement for patients who received pembro over placebo = 37% reduction in event free survival. #tnbc #bcsm #BestofBreast23 pic.twitter.com/rXfqxE6Vix
— Total Health | Oncology 📖🔬 (@TotalHealthConf) January 22, 2023
And don’t even get me started on how often TNBC has higher levels of tumor-infiltrating lymphocytes, another indicator of an immune response from the patient. Again, on this one issue, Ms. McLelland doesn’t know what she’s talking about. She also goes on to claim that ivermectin also—conveniently enough—targets HER2, which led me to think: You do know that if a breast cancer overexpresses (makes too much) HER2, by definition it’s not TNBC, right?
As for any published data on the use of ivermectin to treat TNBC, a search of PubMed produced just one article from 2015, which showed that ivermectin could potentially restore sensitivity to the anti-estrogen drug tamoxifen in the TNBC cell line MDA-MB-231 (a cell line that I’ve worked with extensively over the years) and MMTV-Myc mouse TNBC cells in vitro. In other words, it’s a single study in cell culture that does not say anything about ivermectin resulting in TNBC responsiveness to immunotherapy. Let’s just put it this way. Ms. McLelland is flat-out wrong about this, and when I see two statements that obviously wrong about something I know a lot about (e.g., TNBC is not immunogenic and sensitive to immune therapy and that ivermectin makes these “cold” tumors “hot”), I immediately wonder what other wrong statements she’s making. In fairness, there are studies examining cell culture and animal models of various cancers that show that ivermectin can apparently inhibit the motility in vitro and metastasis in a mouse model of some cancer cell lines and inhibit EGFR signaling (which stimulates cancer growth), but that’s a long way from any good clinical evidence and just shows how cancer quacks like to cherry pick in vitro data and represent it as meaning a treatment works. (For instance, one of these studies used estrogen receptor-positive cells, not TNBC.) I also noticed immediately that these studies used very high concentrations of ivermectin, just like the in vitro studies testing ivermectin against SARS-CoV-2.
So what about Ms. McLelland’s story? She was diagnosed with cervical cancer in 1994 at age 30 and “did all the normal stuff, chemoradiotherapy” and what sounds like a radical hysterectomy. Sadly, this was before she had married and rendered her unable to have children. In 1999 the cancer recurred in her lungs, but in the meantime her mom was diagnosed with stage IV breast cancer, which had led her to look for treatments. This search had led her to one of the favorite areas of cancer abused by cancer quacks, the Warburg effect, or aerobic glycolysis. (Remember dichloroacetate, anyone?) She also developed leukemia, that was apparently attributed to her cancer treatment.
Here I must note a couple of things. First, it is true that stage IV cervical cancer is usually incurable. However, around 15% of patients with stage IV disease can survive more than five years, although it could well be a much lower percentage after a recurrence. Look at it this way. Even if it’s only 1% of patients with recurrent cervical cancer who survive more than five years, the far more likely explanation for Ms. McLellan’s good fortune and continued survival is that she was fortunate enough to be one of these lucky few who survived, not that she somehow through trial and error stumbled onto a regimen of old repurposed drugs—including dipyridamole (Persantine, a drug that I haven’t dealt with in decades), statins, naltrexone, metformin, and others—that cured her. (Actually, clearly even she doesn’t think she’s cured, as she’s still taking them and appears to be adding to the regimen fairly regularly.) Whatever the case, she relates about how a cocktail of “kitchen sink” drugs led to remission and that she is still taking these drugs. This is how her story as touted on Dr. Lawrie’s Substack is a “bait-and-switch.” Ms. McLelland never actually appears to have treated her cancer with ivermectin as far as I can tell from the interview, although she did use it to treat her COVID-19, and even if she did she used it decades after she had a cancer recurrence.
Whenever I hear a “miracle cure” testimonial like this, particularly from someone who has been promoting her “miracle cure” since the late 1990s, I wonder: Why is there no evidence other than the anecdote? Why hasn’t this regimen been studied? Why aren’t there publications showing how effective it is? (Ms. McLelland’s book describing how she “did her own research” doesn’t help.) I also found it odd how little she mentioned her leukemia afterward, given that when she mentioned it she seemed to be saying that it was the more “incurable” of her two cancers. Unsurprisingly, a lot of cancer quackery tropes are in this interview, including the hoary, ever-popular claim that sugar “feeds” cancer, even to the point where near the middle of the interview Ms. McLelland and Dr. Lawrie complain about how hospitals often raise money using bake sales selling “sweet things” and how discordant that supposedly is. (How many times have I heard this before?)
Ms. McLelland also complains that cancer cell metabolism is not taught in our training, which might have been true 30 years ago but most definitely is not true now—nor has it been for a long time. Indeed, back around 2010 I marveled at how targeting the Warburg effect seemed to be the dominant theme at cancer meetings like the American Association for Cancer Research (AACR) and the American Society of Clinical Oncology (ASCO), the two biggest cancer professional organizations in the country, the former dedicated more to basic and translational science and the latter to clinical research. Then, as I went to these meetings year after year, the Warburg effect faded in prominence as other targets rose, such as—you guessed it—immunotherapy with immune checkpoint inhibitors like pembrolizumab. Nor was this because “They” were trying to keep you from knowing about ketogenic diets, targeting tumor metabolism, and the like as treatment modalities. Rather, it’s because the results didn’t quite live up to the hype. It reminded me of how a decade before that even, targeting tumor angiogenesis (the growth of new blood vessels to feed the tumor) dominated these meetings but, as drugs that blocked that process increasingly showed themselves, while effective, not to produce the near-miraculous results observed in mice in the 1990s, oncologists and oncology researchers integrated them—e.g., Avastin—into standard cancer care and started looking for new molecular targets.
None of this stops these two from repeating the same old cancer quack complaints (which are the same complaints of COVID-19 quacks about ivermectin) that “They” (pharmaceutical companies) don’t want you to know about these cheap, safe, and supposedly highly effective treatments for cancer and that Ms. McLelland had succeeded where oncology had failed:
Diagnosed with terminal cancer in the prime of her life, and with no viable treatment options, she used herself as a human guinea pig, putting together a cocktail of low toxicity drugs, not normally used for cancer, alongside a low glycaemic diet and powerful supplements. These ‘starved’ her cancer of glucose, glutamine and fat, which she demonstrates with her ingenious, easy-to-follow ‘McLelland Metro Map’.
Which brings me to ferroptosis.
Ferroptosis
Ms. McLelland’s hyping of ferroptosis as target for cancer therapy caught my interest because it was a rehash of the same quack narrative about sugar “feeding” cancer, namely that you don’t want to consume a lot of iron because it “feeds” cancer cells. Unsurprisingly, it turns out that ferroptosis is more complicated than what Ms. McLelland describes, in which you somehow get cancer cells to release ferritin (a protein-iron complex) and then oxidize it in order to attack the cells by using high dose vitamin C or use old rheumatoid arthritis drugs to induce ferroptosis.
Basically, ferroptosis is a form of programmed cell death that depends on iron. It is, of course, true that targeting ferroptosis in cancer is a hot research topic right now. Indeed, I did a PubMed search for just the year 2022 and came up with close to 500 references, and a Nature Reviews Cancer article from last year notes:
Ferroptosis, as a unique cell death mechanism, has sparked great interest in the cancer research community as targeting ferroptosis might provide new therapeutic opportunities in treating cancers that are refractory to conventional therapies. In recent years, substantial progress has been achieved in understanding the role of ferroptosis in tumour biology and cancer therapy. On the one hand, multiple cancer-associated signalling pathways have been shown to govern ferroptosis in cancer cells14. The engagement of ferroptosis in the activities of several tumour suppressors, such as p53 and BRCA1-associated protein 1 (BAP1), establishes ferroptosis as a natural barrier to cancer development15,16, whereas oncogene-mediated or oncogenic signalling-mediated ferroptosis evasion contributes to tumour initiation, progression, metastasis and therapeutic resistance17,18,19. On the other hand, the distinctive metabolism of cancer cells, their high load of reactive oxygen species (ROS) and their specific mutations render some of them intrinsically susceptible to ferroptosis, thereby exposing vulnerabilities that could be therapeutically targetable in certain cancer types20,21,22,23,24. Furthermore, some cancer cells appear to be particularly dependent on ferroptosis defence systems to survive under metabolic and oxidative stress conditions; consequently, disruption of those defences would be fatal to such cancer cells while sparing normal cells9. These recent data suggest that ferroptosis represents a targetable vulnerability of cancer in certain contexts. Ferroptosis has also been recognized as a critical cell death response triggered by a variety of cancer therapies, including radiotherapy (RT), immunotherapy, chemotherapy and targeted therapies25,26,27,28. Thus, ferroptosis inducers (FINs) hold great potential in cancer therapy (Box 1), especially in combination with conventional therapies25,29,30.
I recommend that those of you with the background to understand this review take a look. For lay people, suffice to say that what Ms. McLelland says about ferroptosis is sort of correct in some parts—e.g., it is true the catalysis by iron of the oxidation of lipids in the cell membrane is a trigger for ferroptosis—but vastly exaggerated. There is so much more complexity to the process, as the review quoted above discusses. Just take a look at this illustration from the article to get an idea:
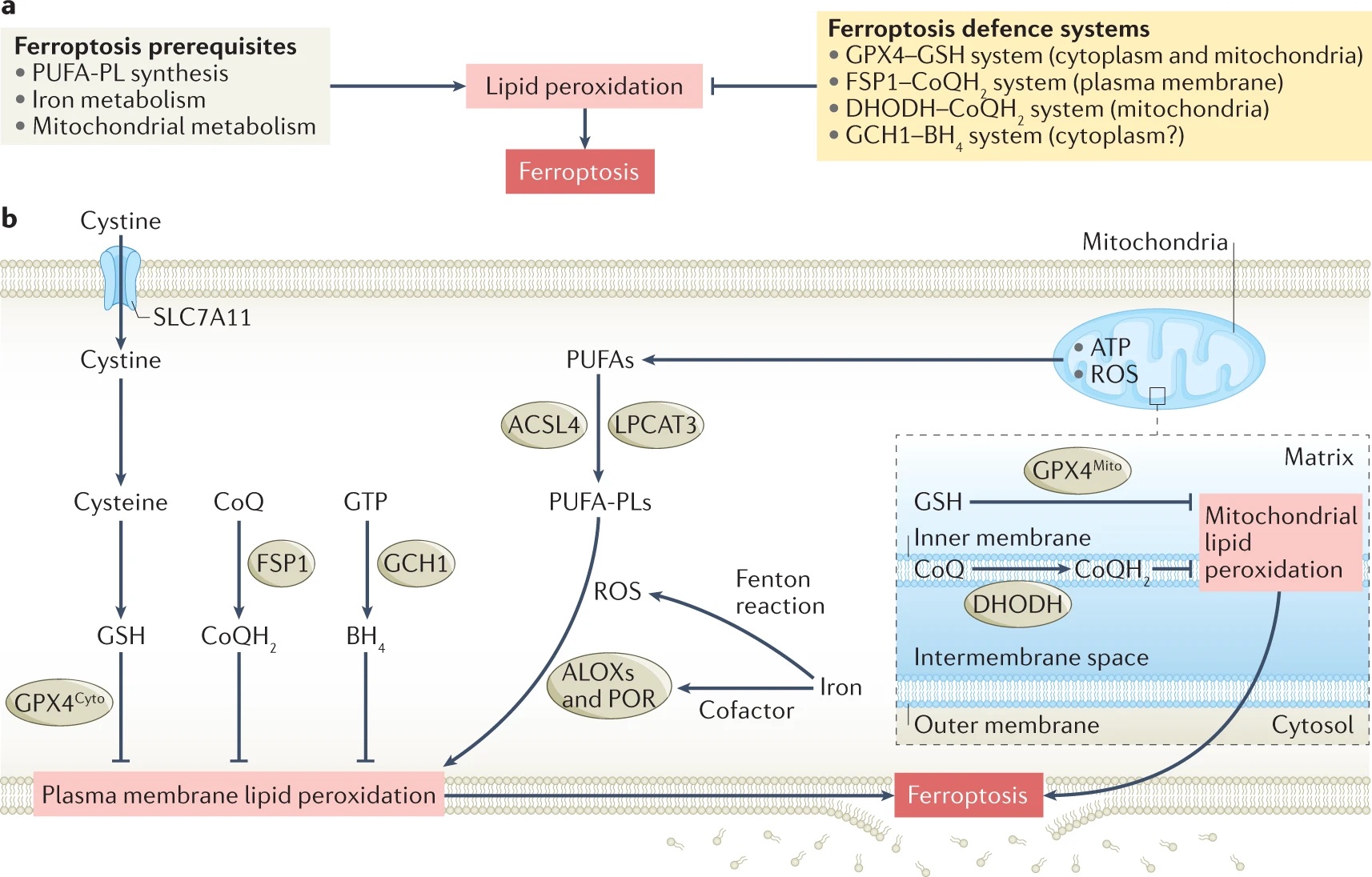
Fig. 1: a | Ferroptosis reflects an antagonism between prerequisites for ferroptosis and ferroptosis defence systems. The prerequisites for ferroptosis consist of polyunsaturated fatty acid-containing phospholipid (PUFA-PL) synthesis and peroxidation, iron metabolism, and mitochondrial metabolism. Ferroptosis defence systems mainly include the glutathione peroxidase 4 (GPX4)–reduced glutathione (GSH) system, the ferroptosis suppressor protein 1 (FSP1)–ubiquinol (CoQH2) system, the dihydroorotate dehydrogenase (DHODH)–CoQH2 system, and the GTP cyclohydrolase 1 (GCH1)– tetrahydrobiopterin (BH4) system. When ferroptosis-promoting cellular activities significantly exceed the detoxification capabilities provided by ferroptosis defence systems, a lethal accumulation of lipid peroxides on cellular membranes lead to subsequent membrane rupture and ferroptotic cell death. b | Acyl-coenzyme A synthetase long chain family member 4 (ACSL4) and lysophosphatidylcholine acyltransferase 3 (LPCAT3) mediate the synthesis of PUFA-PLs, which are susceptible to peroxidation through both non-enzymatic and enzymatic mechanisms. Iron initiates the non-enzymatic Fenton reaction and acts as an essential cofactor for arachidonate lipoxygenases (ALOXs) and cytochrome P450 oxidoreductase (POR), which promote lipid peroxidation, and mitochondrial metabolism promotes the generation of reactive oxygen species (ROS), ATP and/or PUFA-PLs. Excessive accumulation of lipid peroxides on cellular membranes can trigger ferroptosis. Cells have evolved at least four defence systems with different subcellular localizations to detoxify lipid peroxides and thus protect cells against ferroptosis, wherein cytosolic GPX4 (GPX4cyto) cooperates with FSP1 on the plasma membrane (and other non-mitochondrial membranes) and mitochondrial GPX4 (GPX4mito) cooperates with DHODH in the mitochondria to neutralize lipid peroxides. The subcellular compartment in which the GCH1–BH4 system operates remains to be defined. CoQ, coenzyme Q (also known as ubiquinone); SLC7A11, solute carrier family 7 member 11.
Any similarity between Ms. McLelland’s simplistic take and the complexity above is mainly by coincidence only. Indeed, I want to call her version of ferroptosis “ferrobabble,” a nod to the term “technobabble” in Star Trek, the same way I refer to quacks invoking the immune system as spouting “immunobabble.” As an aside, I’ve written a couple of—as yet unfunded, alas—grants looking at targeting the cystine transporter SLC7A11 in order to induce ferroptosis using a repurposed drug. That’s one reason why I laughed listening to these two women say that no one is interested in repurposed drugs. Lots of investigators are interested in repurposed drugs and derivatives of repurposed drugs to treat cancer. This has been true ever since I first met up with a surgeon and a basic scientist who were researching the repurposed drug that I’ve published on.
Unsurprisingly, near the end of the interview, Ms. McLelland relates how she had been “pressured” to take the COVID-19 vaccines, first a non-mRNA vaccine and then two doses of an mRNA vaccine, after which she resisted getting a second booster. Then she got COVID-19 and—surprise! surprise!—got better almost immediately after a single dose of ivermectin. Also, her regimen has supposedly cured her “late onset cystic fibrosis,” because of course it has.
Again, I’m happy that Ms. McLelland is continuing to do well and remains, as far as we know, cancer-free. However, as much as I don’t want anyone to die of cancer, that doesn’t mean that I won’t, when I see a believer who thinks she’s cured herself of a deadly disease with quackery turn around to start promoting and selling that quackery, hold back on calling it quackery and explaining why. Think, for example, Chris Wark of “Chris Beat Cancer” fame. (He did beat cancer, but it was the surgery, not the quackery, that saved him.)
Crank magnetism or crank expansion?
Long before the pandemic, we were discussing cases of how “single issue” cranks and quacks seemed almost inevitably to embrace more and more forms of pseudoscience, conspiracy theories, and quackery. In a way, I think this might well be a related, but distinct form of crank magnetism that I like to refer to as, “Come for one conspiracy theory, stay for conspiracism.” We’ve seen so many examples of this phenomenon, too, beginning with how COVID-19 minimizers and the conspiracy theorists who thought it was a “plandemic” or “bioweapon” soon embraced all manner of other conspiracy theories and pseudoscience, including conspiracy theories involving antivaccine activism, QAnon, antisemitic conspiracy theories, big pharma supposedly suppressing “miracle cures” that “They” don’t want you to know about. Just look at how, for example, Drs. Robert Malone, Pierre Kory, Peter McCullough, and the whole crew of “America’s Frontline Doctors,” among many, many others, have expanded from their single issue “alternative treatments” for COVID-19 to embrace pretty much every conspiracy theory about COVID-19 that there is, including those of “depopulation” and “died suddenly” (of the vaccine) and political conspiracy theories involving how Russia is not the aggressor in Ukraine. Similarly, “old school” antivaxxers like Joe Mercola and Robert F. Kennedy, Jr. have eagerly glommed onto the new COVID-19 conspiracy theories and “miracle cures.” There seems no end to their “magnetism” for crankery.
Dr. Lawrie started out, as far as I can tell, mainly as a believer in ivermectin as a cheap, safe, and highly effective treatment for COVID-19, but then gradually (or not so gradually) embraced more and more pseudoscience until now she’s promoting cancer quackery of the sort that Ms. McLelland has been peddling since the 1990s. Ms. McLelland, in the meantime, has naturally glommed onto ivermectin as the new “in” drug among the COVID-19 conspiracy crowd.
Crank magnetism marches on.